Published On January 2, 2015
IN ADDITION TO BEING A MARVEL OF ENGINEERING AND, according to its proponents, a harbinger of the future of surgery, the da Vinci robotic surgery system is just plain cool. Even watching a video of a procedure in Ashutosh Tewari’s ninth-floor office at Weill Cornell–New York Hospital in Manhattan requires special equipment. “Put these on,” Tewari says, handing over a pair of 3-D glasses not unlike those distributed to audiences at science-fiction movies during the 1950s.
On the screen, the lower abdominal cavity of a man undergoing a radical prostatectomy—removal of a cancerous prostate—is illuminated like the interior of an animated red-walled cave. About the size of a walnut, the prostate gland, which produces seminal fluid, is located under the bladder and surrounds the urethra. Removing it is a delicate procedure, compounded by the gland’s proximity to bundles of nerves and tissues controlling continence and sexual function. In the video, tiny silver forceps, the size of a dime, gently clasp pieces of fibrous tissue enclosing the prostate, while miniature scissors carefully snip away, slowly exposing the prostate. Finally, the offending gland is cut off and removed. With movements just as delicate and precise, the urethra, which had to be cut along with the prostate, is surgically reattached to the bladder.
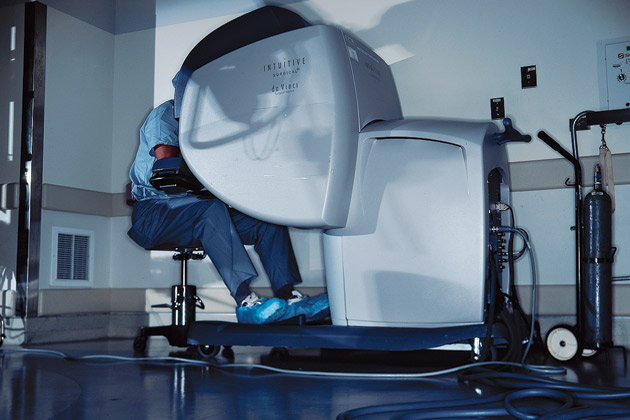
What isn’t visible on the video are the fingers of Tewari, a urologic oncologist and director of Weill Cornell’s robotic prostatectomy program. That’s because, instead of bending over the patient, as in conventional surgery, Tewari remained on the other side of the room, peering through a 3-D viewer while manipulating the robot’s controls with his hands and feet.
During a robotic prostatectomy, only support personnel—nurses, an anesthesiologist and a surgical assistant—stand near the patient. In place of the surgeon’s hands are robotic arms, angling down toward the patient. At the surgeon’s instruction, the assistant carefully inserts the slender rods at the ends of the robotic arms into five small incisions forming a semicircle on the patient’s abdomen. Each rod carries a separate tool—forceps, scissors, various blades—which the surgeon manipulates at the console, each hand movement precisely mimicked inside the patient. The machine softens any unintentional hand motions or tremors, while the surgeon’s foot controls the camera arm. The image is magnified 10 times, with side-by-side lenses creating a 3-D view. Because the console is connected to the robotic arms only by wires, the surgeon, with the proper electrical connections, could be in another room—or another country.
The robot at Weill Cornell is one of 382 in the United States, and 509 worldwide, as of late 2006, all of them manufactured by Intuitive Surgical of Irvine, Calif. Dubbed da Vinci (to honor Leonardo da Vinci, who designed a robot more than 500 years ago), it is the only surgical robot currently in use. The Food and Drug Administration approved the da Vinci for radical prostatectomies in May 2001, and it has caught on rapidly, now handling more than a third of those procedures in this country, compared with just 2% in 2002. Since 2001, the da Vinci has also been approved for several other procedures, including mitral valve repairs and cystectomies.
Tewari and other proponents think the da Vinci is a leap toward less invasive surgery. Traditional open prostatectomy requires an eight- to 10-inch incision and a hospital stay of several days, with possible blood loss during the procedure, significant post-operative pain and a lengthy at-home recovery. Laparoscopic surgery, in which a surgeon manually inserts and manipulates miniaturized tools through small incisions, can minimize pain and hospital stays, but the tools are difficult to control, and the procedure requires such a high level of training that relatively few surgeons offer it for prostatectomies and other comparably complex procedures. In contrast, most surgeons who try the da Vinci find that its technological advantages let them perform minimally invasive surgery with relative ease.
Skeptics, though, while marveling at what robotics seems to offer, worry that hype is outpacing reality, pushing hospitals to invest in expensive technology before its benefits have been established. What’s needed, they say, are more randomized, controlled tests of the sort used to validate other kinds of medical advances. Yet, while several such studies are under way, many hospitals worry that they can’t wait for the results. Often pressed by staff physicians to provide the latest technology, the institutions must base their decisions on little more than educated guesses.
A surgical robot can dent the budget of even the most financially secure institution. In addition to the purchase price—$1.5 million for the latest model—a da Vinci requires extra personnel in the operating room, an annual maintenance fee of $100,000 after the first year and a host of “disposables,” instruments that can be used just once or only a few times before being replaced. That alone adds $1,500 or more to the cost of performing a procedure. Unless a hospital can devote an operating room solely to robotic surgery, there are also costs to set up and take down the machine between uses. Meanwhile, most insurers pay a flat rate for a procedure, regardless of whether it is performed using open, laparoscopic or robotic techniques.
Of course, the more you use an expensive piece of equipment, the more economically viable it becomes. Tewari performs about 300 prostatectomies a year. He says that sitting at the console, in a relaxed position, enables him to do more procedures than he could if he were standing upright over a patient. And because reimbursements are the same regardless of how long a patient is in the hospital, shorter stays should save money, to the tune of the hundreds of dollars a night it costs for an inpatient bed. “If you get a patient who would have been in the hospital three days out in just one day, you essentially have three times the beds,” Tewari says.
A hospital then can handle more patients and receive more reimbursement. And there are other benefits too. Less loss of blood means less stress on the blood bank, and robotic-surgery patients tend to be pleased with their results. Weill Cornell is getting so much use out of its one da Vinci robot that it is considering buying a second, says E. Darracott Vaughan, chairman emeritus of the urology department and a force behind the hospital’s adoption of robotic surgery.
Hospitals that manage to keep their surgical robots busy tend to be big supporters of the technology. Hackensack University Hospital in New Jersey now has four da Vincis, and surgeons there, in addition to performing prostatectomies, increasingly turn to the robot to perform another delicate procedure—colectomy, the removal of a section of a diseased colon. Last summer, addressing a robotic-surgery conference in New York City, Hackensack surgeon Garth H. Ballantyne asserted that “there is no question anymore that laparoscopic colectomy is superior to open colectomy.” Yet because of the difficulties posed by laparoscopic procedures, Ballantyne said, “there are few people who are doing it. So I believe that robotic surgery is the solution.”
Nevertheless, other administrators, particularly at smaller hospitals, hesitate to break the bank. At Mercy General Health Partners, a 282-bed facility in Muskegon, Mich., the issues surrounding a potential purchase came into sharp focus last summer after a competitor, Hackley Hospital, got a da Vinci. Mercy General officials ultimately decided to pass after determining that the local population would generate, at most, 50 to 100 robotic-surgery candidates per year.
IT WOULD BE EASIER TO SPRING FOR a $1.5 million robot if you knew for sure it represented a clear step forward. Yet while FDA trials have concluded that the da Vinci is safe and effective for a growing number of surgical applications, so far there is little data addressing whether, in fact, robotic surgery is superior to open or laparoscopic procedures. In 2003, one study by a team at Vattikuti Urology Institute at Detroit’s Henry Ford Hospital found that 100 patients undergoing robotic prostatectomy lost less blood than 100 who had open surgery and 50 who got nonrobotic laparoscopic procedures. And hospital stays after robotic surgery were shorter—1.2 days on average vs. 3.5 for open surgery and 1.3 for laparoscopic.
But the study touched only briefly on complications of prostatectomy such as incontinence and impotence, and it didn’t address whether da Vinci patients had a lower incidence of such problems. In another study at Henry Ford, 97% of 154 patients who had robotic prostatectomies reported the return of sexual function, a result surgeons attribute largely to the da Vinci’s magnified view and precise motions. Yet, while an October 2006 paper in the British Journal of Urology called such studies promising, it noted that “clearly, data from so few patients need to be treated with caution, and outcomes from one specialist centre might not always be achievable elsewhere.”
It’s also too early to know whether the da Vinci offers improvements in long-term patient outcomes. For patients with prostate cancer, open radical prostatectomy is considered the gold standard, much more widely available than laparoscopic prostatectomy and offering the best chance of patient survival over five to 10 years. How does the da Vinci compare? There are no studies to answer that question. “A rigorous scientific process needs to be gone through before one can figure out whether a certain technology is better than another, and that hasn’t been done,” says W. Scott McDougal, chief of urology at the Massachusetts General Hospital (MGH) and Walter S. Kerr Jr. Professor of Urology at the Harvard Medical School.
At many hospitals, much of the pressure to consider a da Vinci purchase comes from a staff worried about falling behind the technological curve. But in 1997, doctors at Brigham and Women’s Hospital in Boston did more than just lobby for the da Vinci. Hoping to participate in clinical trials for heart valve procedures, cardiac surgeons at the hospital established a “robot fund” to help pay for the machine. Donors, primarily former patients, gave about 20% of what was then a $1.2 million purchase price, and the hospital picked up the rest of the cost.
“We were very interested in this as a technique for minimally invasive valve surgery,” says Lawrence Cohn, former chief of cardiac surgery at Brigham and Women’s. Cohn, who has performed some 2,000 mitral valve repairs, is a leading specialist in the procedure, in which surgeons correct narrowing or leakage of the valve that controls the flow of blood into the heart’s left side. “If you could do an operation of the same quality, with much less trauma, that’s great for the patient,” he says.
But after performing just five successful repairs with the help of the robot, Cohn decided against using a da Vinci. “The operations went very well,” Cohn recalls. “But using the robot required a pretty large logistical team, and it took twice as long to do a repair as when I did it in the usual way.” Cohn concedes that, had they continued to hone their skills on the machine, they would have gotten more efficient. Still, he missed the feel of holding instruments in his hands and working directly on the valve. “It’s a great machine,” Cohn says. “The visualization it provides is incredible. But the complexity of valve pathology didn’t lend itself to consistent repair by the robot.” Nevertheless, the machine won’t sit unused: The hospital recently hired a urologist trained in robotic surgery to employ da Vinci for prostatectomies.
A few miles away, at the MGH, president Peter Slavin has yet to be convinced that the hospital needs a da Vinci at all. “Perhaps the most important benefit, from my perspective, is that the robot is innovative,” Slavin says. “Hospitals, particularly teaching hospitals, have a responsibility to promote innovation. But we can’t do that in every case. We have to be somewhat selective. And so far we haven’t been convinced that this is an opportunity of sufficient value.”
Still, Slavin calls the da Vinci “one of the most interesting case studies of technology adoption I’ve ever encountered. As administrators, we face major decisions every day—about which personnel to hire, and what equipment, drugs and devices to purchase. This is a dramatic example of those decisions.”
A major test of the da Vinci’s value—and that of future robotic devices—will be randomized, controlled tests that can determine how well patients do years after a procedure. If the results can’t match those of open surgery, Cohn says, faster and less painful surgery won’t hold much value. “It’s great to have new technology, but at the end of the day, you’d better have at least as good a result as you did with the old technique, or you’re just kidding yourself.”
Dossier
“Robotics in Urologic Surgery: An Evolving New Technology,” by Fatih Atug et al., International Journal of Urology, July 2006. A comprehensive discussion of the development of robotic surgery.
“Endoscopic robotic mitral valve surgery,” by Douglas A. Murphy et al.,Journal of Thoracic and Cardiovascular Surgery, October 2006.A study that finds robot-assisted surgery to be “safe and effective” for 127 heart patients needing mitral valve repairs.
“Robotic Radical Retropubic Prostatectomy,” by M. Menon, British Journal of Urology, February 2003. A report on open, laparoscopic and robotic surgeries that provides evidence that patients suffer the least blood loss and endure the shortest hospital stays after robotic surgery.